
Decision Neuroscience
Making decisions is part of our daily life
Decision Neuroscience, a branch of Neuroeconomics, combines concepts from behavioral economics, cognitive science and psychology to study how we make decisions.
What is NeuroEconSolutions?
We are a team of scientists committed to improve the understanding of how decisions are made in health care. We apply principles and strategies from behavioral economics and translate them into clinical practice
The conceptualization of our innovative strategy merges two worlds — Neuroeconomics and Medicine.
We work with our clients to identify specific health care issues to bring practical solutions.
Our Founders & Scientific Leaders
Prof. Dr. Gustavo Saposnik is a Neurologist, PhD in Neuroeconomics (Decision Neuroscience) with over 20 years of experience in academic research.
Professor Saposnik is the Founder and Scientific Director of NeuroEconSolutions, an Associate Professor at University of Toronto, and a Staff Neurologist and Scientist at St. Michael’s Hospital.
Dr. Saposnik achieved international recognition as reflected from his passion for research and innovation in this novel field, personal awards, peer-review funding, over 280 publications, and invitations as a keynote speaker in over 20 countries.
Gustavo Saposnik, MD MPH PhD FRCPCFounder and Medical Director

Maria Terzaghi is a Registered Pharmacist who brings over 15 years of experience working in the pharmaceutical industry and also teaching at at the University of Toronto. Maria is one of the founders who provides expertise in Regulatory Affairs, clinical trials design, and graduate and postgraduate education.
Maria is the liaison with our partners, research and marketing teams and leads the operations for the ongoing and prospective studies.
Maria A. Terzaghi, RPhFounder and Director of Operations

Our Research Team
Our work is enhanced by recruiting leaders in artificial intelligence, expert methodologists and trial designers, behavioral economists, statisticians, front-line health care providers, and students.
Many of our team members are internationally recognized leaders in clinical research, education, and clinical practice.
We’ve also partnered with the Decision Neuroscience Lab at the University Of Toronto, the Laboratory for Social and Neural Systems Research at the University of Zurich , the Li Ka Shing Institute at St. Michael’s Hospital, Toronto, and the Stroke Outcomes Research Group (SorCan.ca), among others.
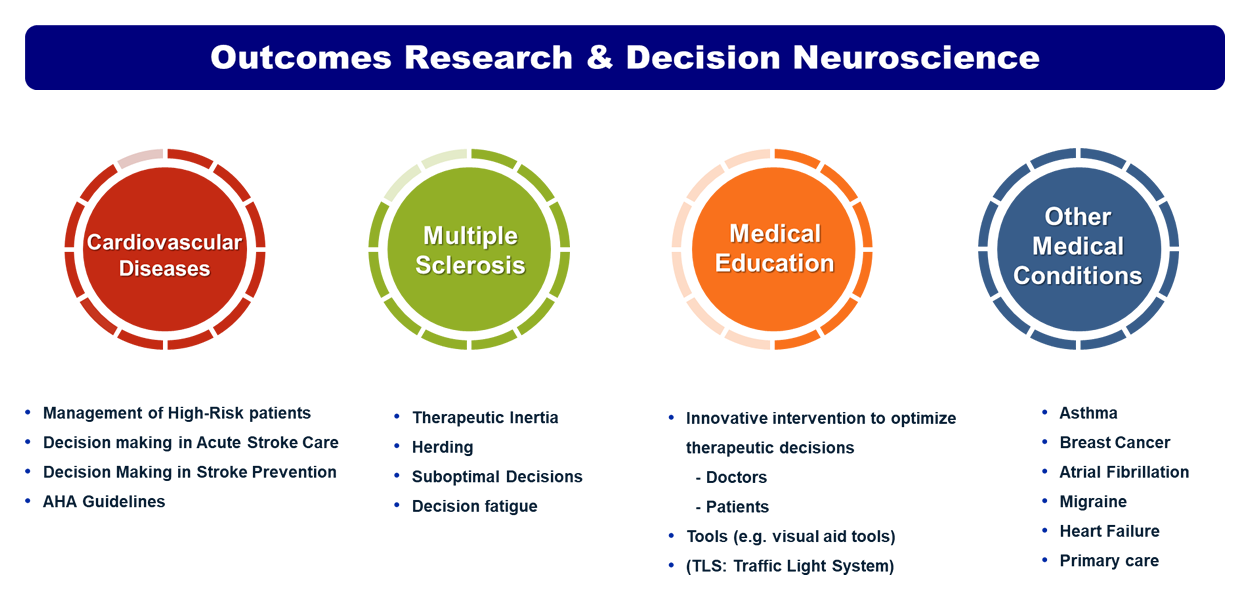
Strategy & Research Focus
Our Strategy Steps

Our Research Focus
Our Mission
To increase awareness about cognitive biases and facilitate optimal decisions of healthcare professionals thru innovative research.
To improve medical education and patients’ experiences and outcomes through innovative research.
Our Goals
To create and evaluate educational interventions targeting health care professionals and patients to overcome therapeutic inertia and status quo
To improve patients’ experiences and outcomes by applying principles from neuroeconomics
To promote the implementation of patient centered outcomes
To identify issues and provide solutions towards a shared decision processes
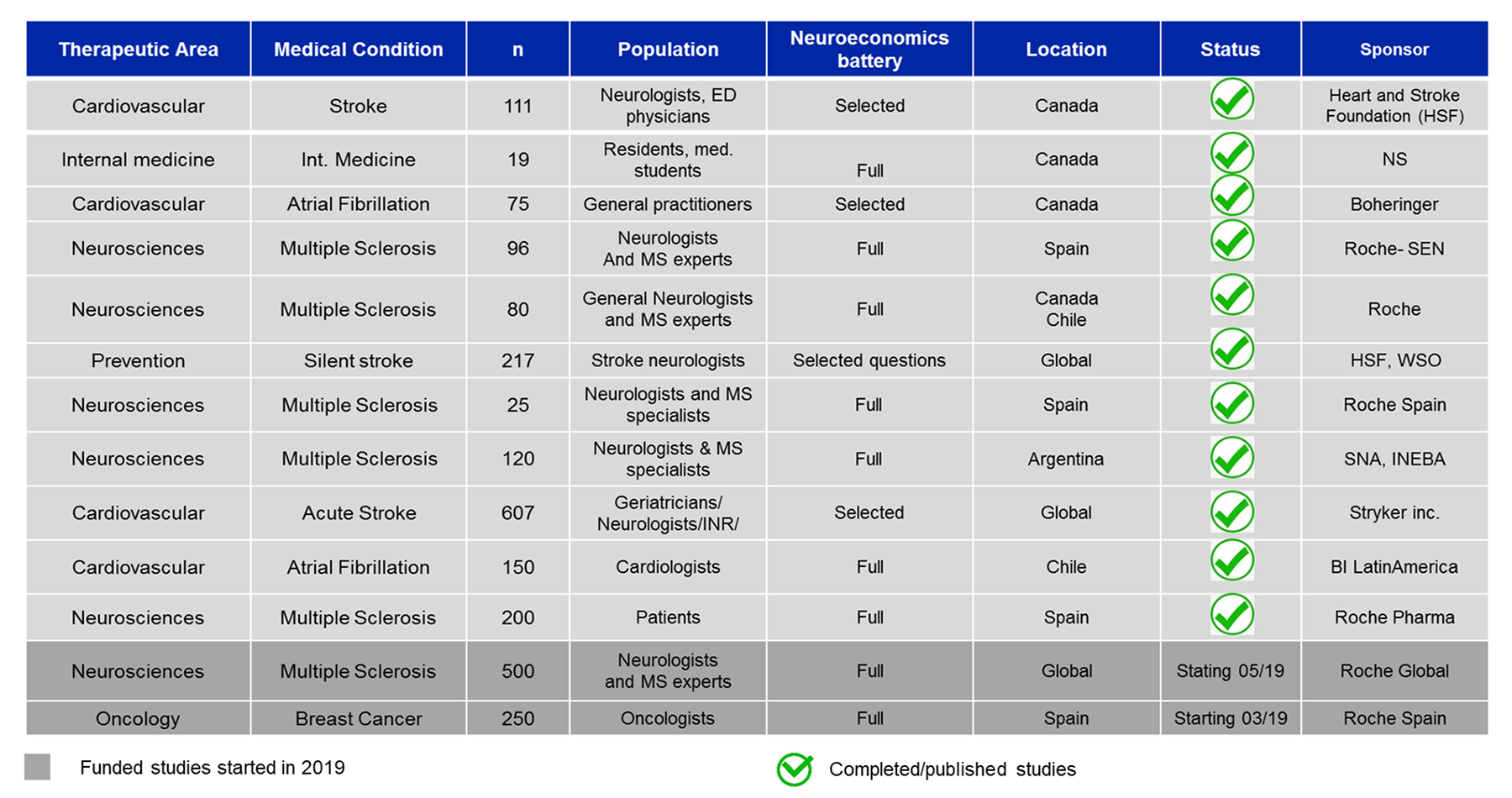
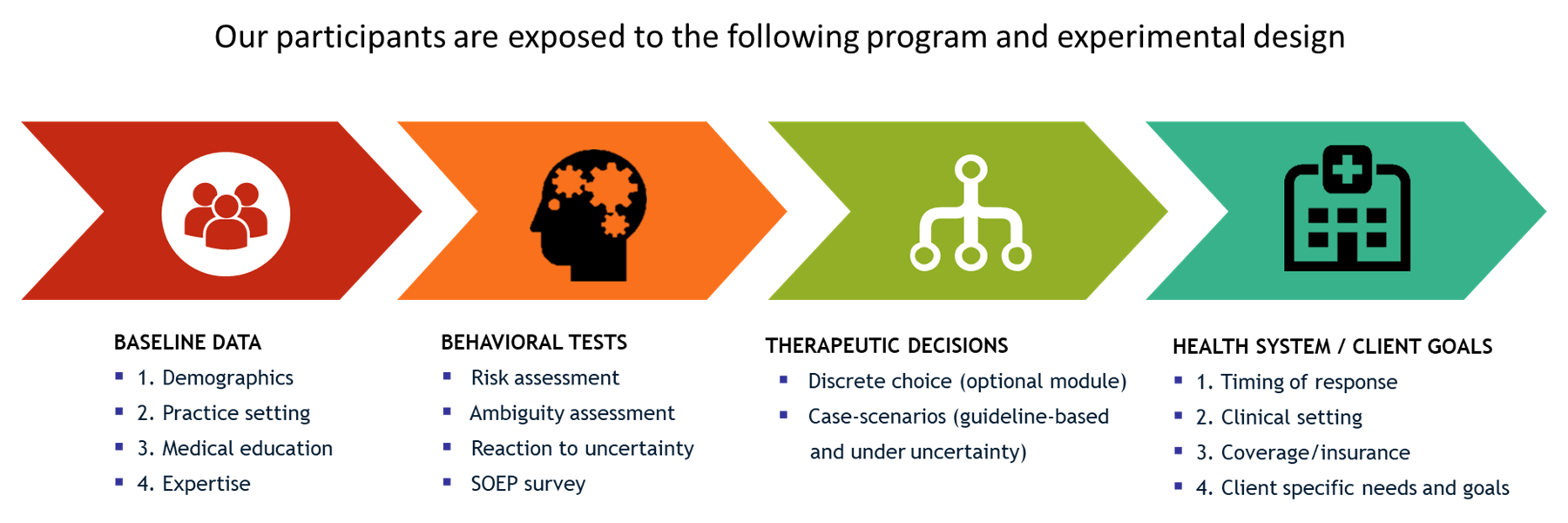
Our Platform

Example 1: Therapeutic Inertia
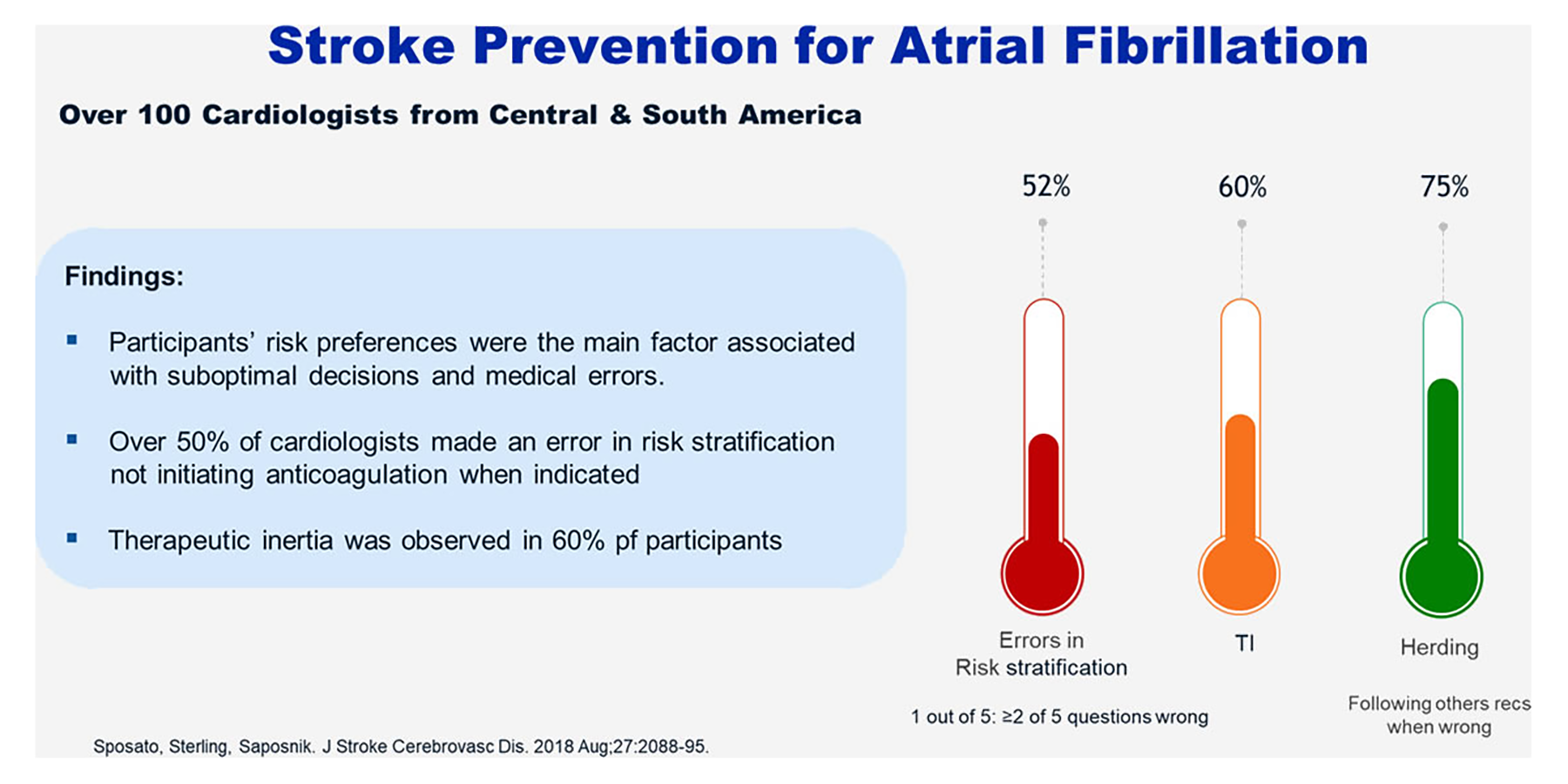
Example 2: Stroke Prevention for Atrial Fibrillation
Example 3: Educational Intervention
Example 4: TI Mechanisms
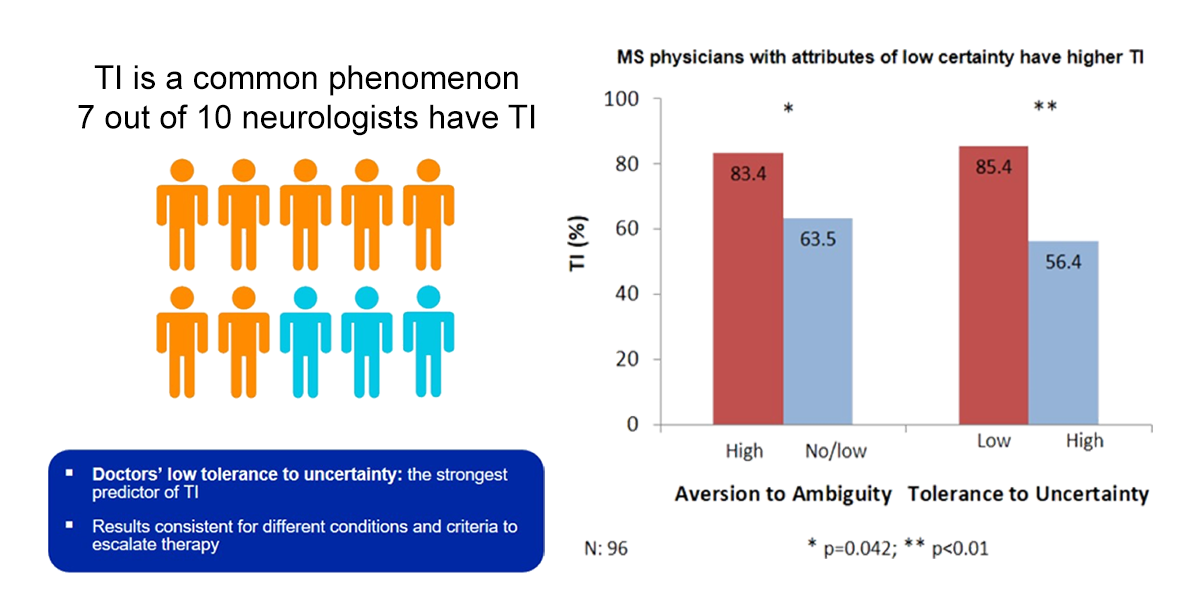
Example 1: Therapeutic Inertia
Therapeutic Inertia (TI): introduced in 2006
- Definition: “absence of treatment initiation or intensification when treatment goals are unmet”
- Consequences: TI Leads poorer patient’s outcomes and suboptimal MS care
- Studies from Europe and North America: >50& patients remained with control hypertension (Wang YR, et al. Arch Intern Med 2007;167:141-147, Grassi G, et. al. Eur Heart J. 2011;32:218-225)
- Early intense MS therapies more effective than escalation therapies (lower EDSS at 5 yrs; p=.002) (Harding K, et al. JAMA Neurol 2019;76(5):536-541)
- Treatment escalation leads to fewer relapses (Relapse rate ratio – 30%; 95%CI 14-44%) (Chalmer et al. J Neurol 2019 Feb;266(2):306-31)
Example 2: Stroke Prevention for Atrial Fibrillation
A Study of over 100 Cardiologists from Central & South America
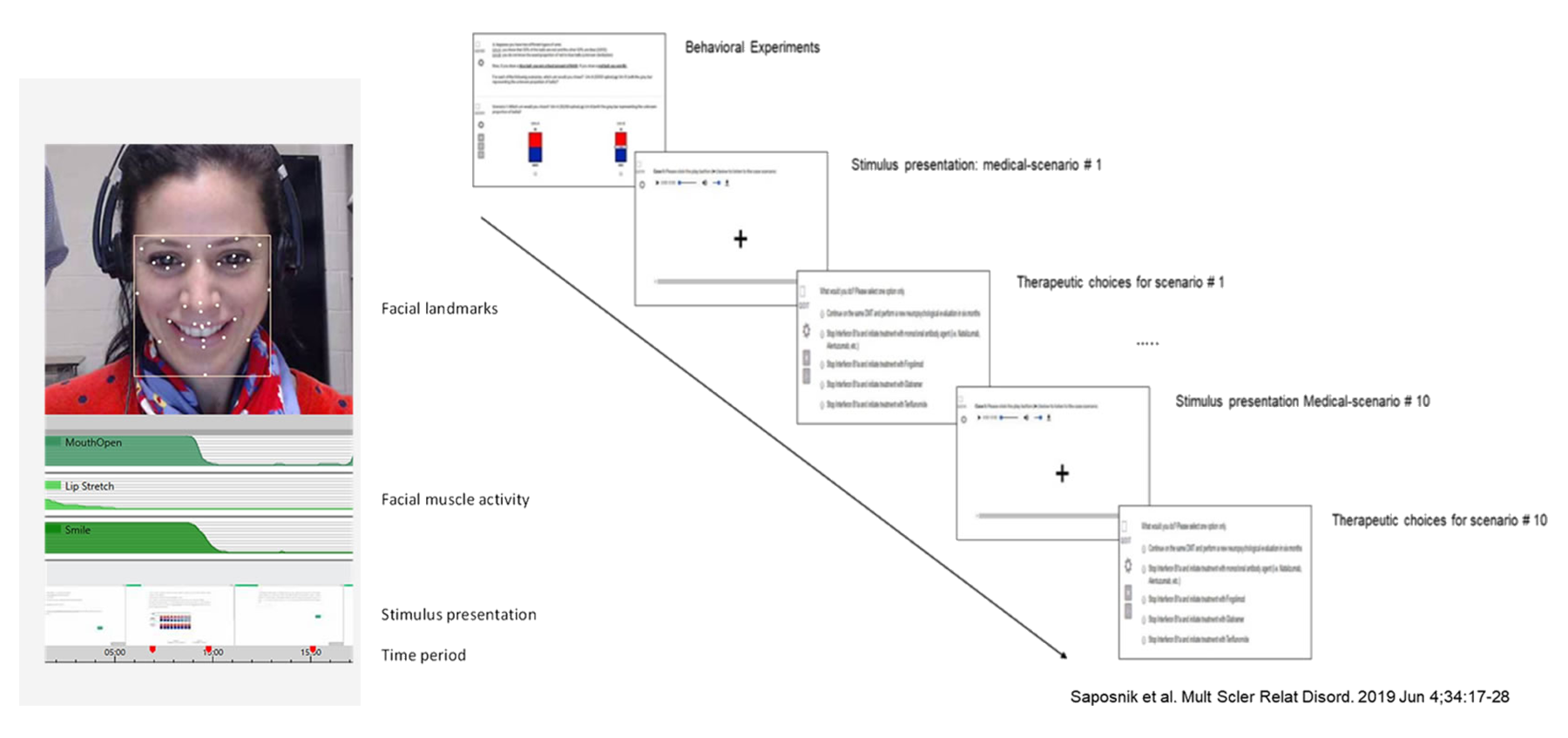
Example 3: Educational Intervention
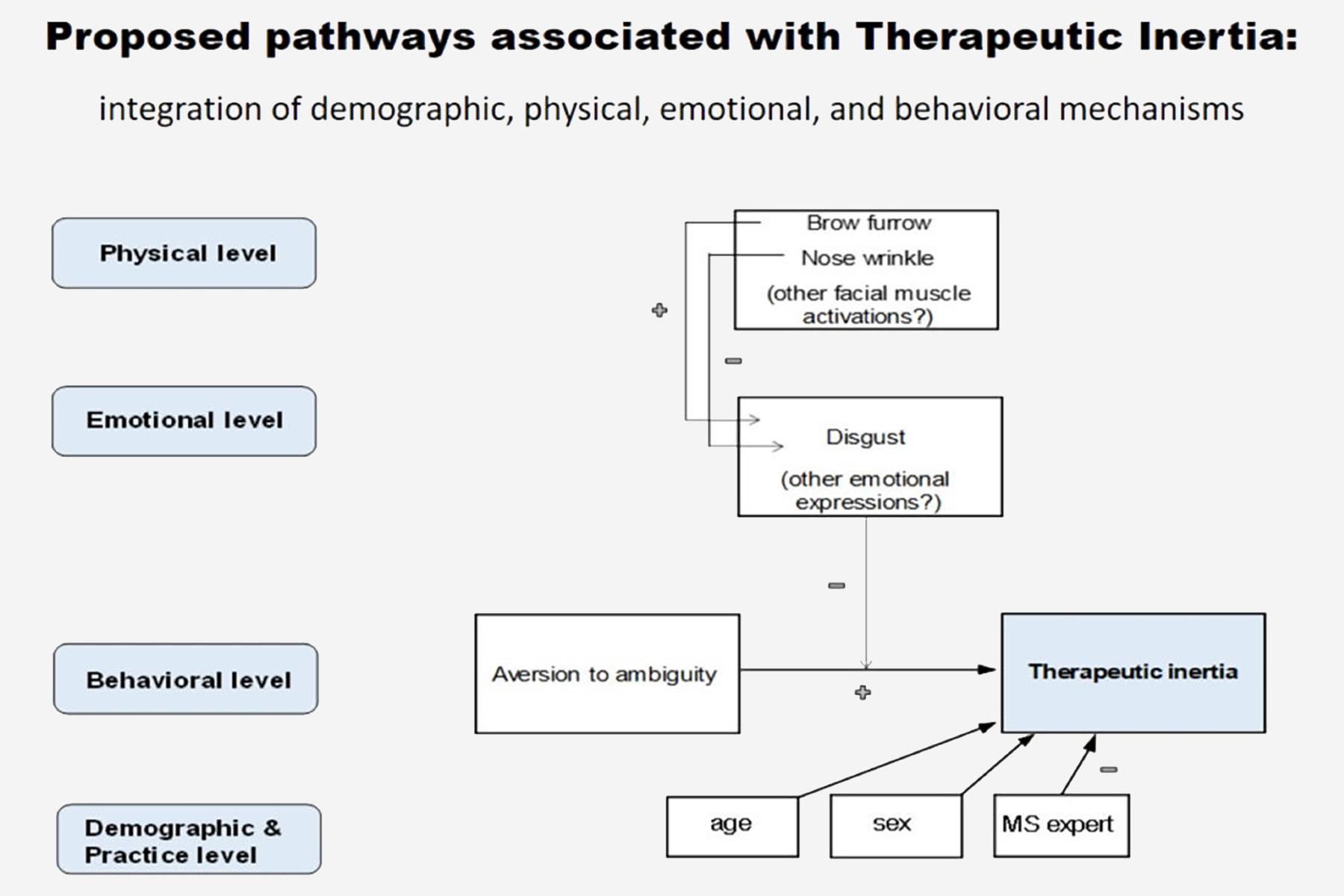
Example 4: TI Mechanisms
Publications
Decision making poker players and neuroeconomics
Making decisions in medical care is a difficult task, involving a variety of cognitive processes. Decision making is defined as the process of examining possibilities, risks, uncertainties, and options, comparing them, and choosing a course of action. Decisions based on erroneous assessments may result in incorrect patient and family expectations, and potentially inappropriate advice, treatment, or discharge planning (eg, longer length of hospitalization, long-term placement, and wasted resources). Rapid and accurate decision making is critical to stroke care, for which several factors have proven effect on outcomes. In brief, there are patient-level, hospital-level, and provider-level characteristics that directly affect stroke outcomes.
![]()
to read full article, please click here
Decision making general concepts in Neuroeconomics
![]() to read full article, click here
to read full article, click here
Emotional Expressions and Therapeutic inertia underlying mechanisms
![]() to read full article, please click here
to read full article, please click here
Factors associated with therapeutic decisions in acute stroke care (UNMASK EVT)
![]() to read full article, click here
to read full article, click here
![]() to read full article, click here
to read full article, click here
The role of uncertainty in therapeutic decisions
![]() to read full article, click here
to read full article, click here
Therapeutic Decisions in Atrial Fibrillation for Stroke Prevention
![]() to read the full article, click here
to read the full article, click here
Therapeutic intertia a comparative study among 4 countries
![]() to read full article, click here
to read full article, click here
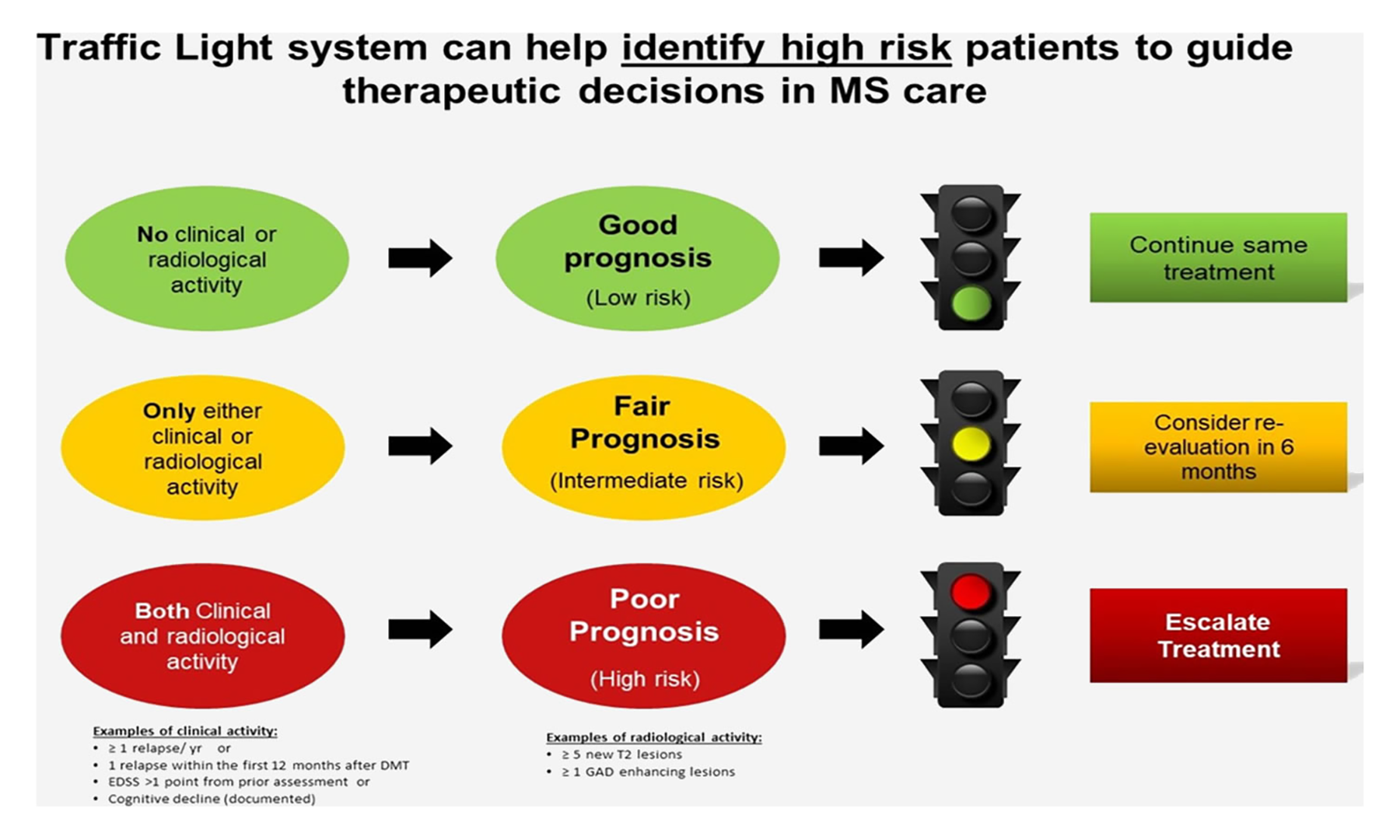
Traffic light system reduces therapeutic inertia: A proven effective educational intervention
![]() to read full article, click here
to read full article, click here
What do we know about Therapeutic Inertia? Lessons learned from Neuroeconomics
![]() to read full article, click here
to read full article, click here